Medical Liturgy
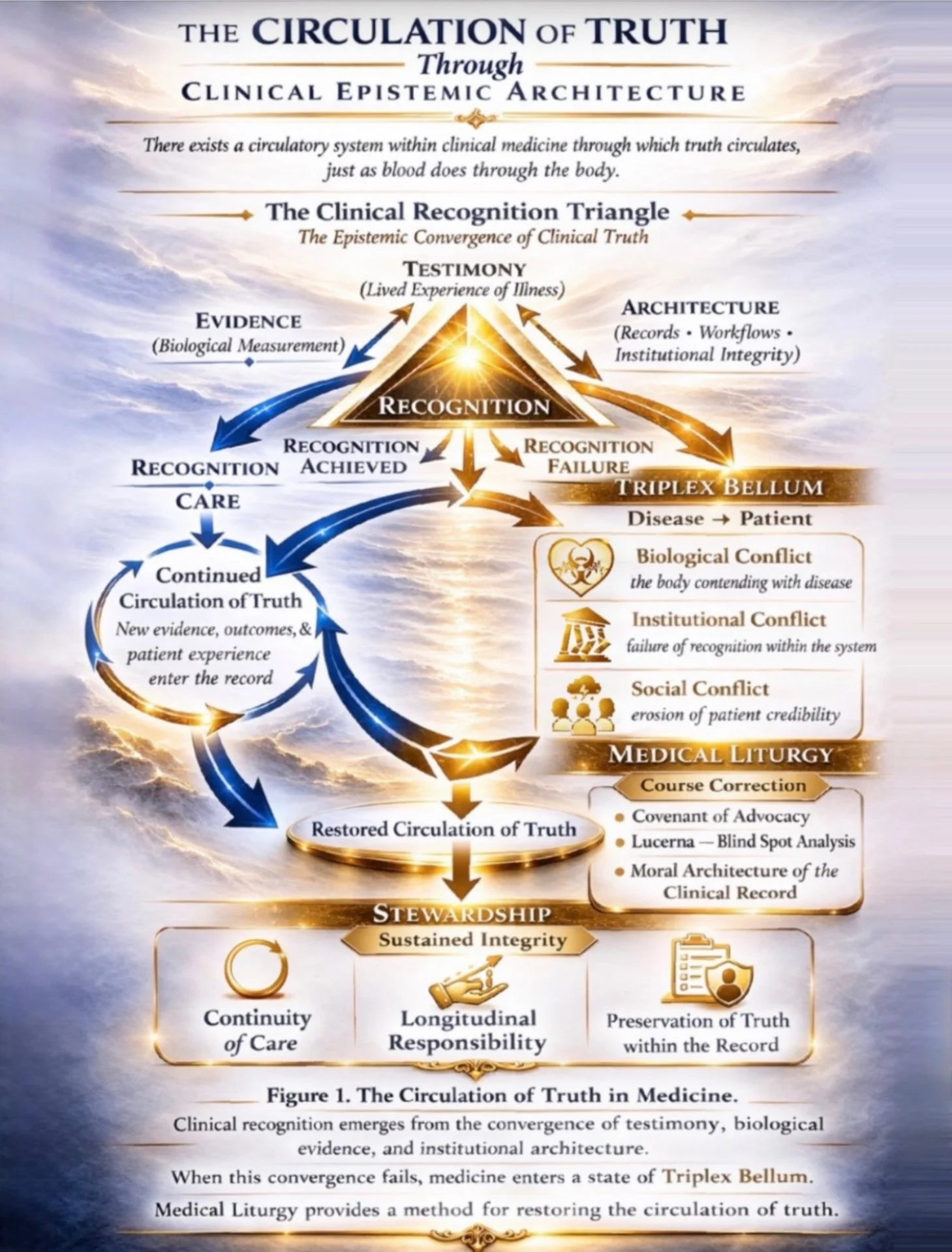
The Circulation of Truth Through Clinical Epistemic Architecture
For the Moral Body What Harvey Did for the Physical One
Studies in Narrative, Ethics & Evidence
The Architecture of Record
There are forms of suffering that do not disappear because they are absent.
They disappear because they are not carried forward.
A symptom may be documented.
A scan may be performed.
A testimony may be spoken clearly and in full.
And still, what is present may fail to remain visible long enough for recognition to occur.
This is the problem of record.
Not merely whether something was written down,
but whether it was preserved, transmitted, interpreted, and carried across time with enough continuity to become care.
At that threshold, documentation becomes more than storage.
It becomes structure.
Evidence enters the record.
Testimony enters the record.
But what enters the record does not always survive the systems meant to hold it.
To understand how truth about illness moves —
how it converges, fragments, disappears, or reaches recognition —we must begin with circulation.
“It is possible—no, essential—to walk through something both sacred and unbearable. To hold in one hand the lexicon of science and in the other the quiet grammar of prayer. To keep belief and verification from tearing each other apart. To measure the invisible and still bow before it.”
- C L Gillespie
Medical Liturgy
medica liturgia
n. · adj.
A discipline studying how truth about illness circulates through clinical epistemic architecture. Evidence and testimony emerge as signals of illness, but those signals must travel through institutional systems before recognition can occur. When circulation succeeds, recognition emerges and care follows. When circulation fractures, recognition collapses even though evidence and testimony remain present. The framework therefore examines the structures that allow clinical truth to move, converge, and remain visible long enough for care to occur.
A first principle of ordered care: that by which what is present is not permitted to pass through the system without recognition.
Etymologia
Medical
medicus, medicina, mederi
to heal; to treat; to attend
Etymologia Profunda
med-
to measure; to consider; to give counsel; to take appropriate action
Ratio
Medical does not begin with cure.
It begins with measure.
What is present must first be brought into proportion.
What is brought into proportion may be recognized.
What is recognized may be carried forward.
Where measure fails, recognition does not occur.
Where recognition does not occur, care does not follow.
Definitio
Medical
the disciplined act by which what is present is measured, discerned, brought into recognition, and made available for care.
Liturgy
leitourgia
laos – the people
ergon – the work
public work; service undertaken on behalf of the people; obligation borne for the maintenance of common order
Ratio
Liturgy is not ceremony.
It is structure.
It is the work required to maintain the conditions under which recognition remains possible.
Where it holds, continuity is preserved.
Where continuity is preserved, what emerges remains gathered.
Where it fails, what is present disperses before it can be recognized.
Definitio
Liturgy
the public duty of maintaining the structures through which what is present remains visible, gathered, and capable of recognition.
Compositio
Medical – that which measures and brings into recognition
Liturgy – that which preserves the conditions for recognition and prevents dissipation
Medical Liturgy
the public duty of preserving the structures of recognition
through which measurement becomes recognition
and recognition becomes care.
Ordo
Where there is suffering, there are signs.
Where there are signs, there must be gathering.
Where there is gathering, there must be measure.
Where there is measure, there must be recognition.
Where there is recognition, there must be care carried forward.
Where this order is broken, truth may remain present without recognition.
Scholium
Evidence may persist.
Records may accumulate.
Images may be obtained.
Yet still:
presence of evidence
is not the same as recognition.
Thus it is held:
failure of care
is not always absence of evidence,
but absence of recognition.
Axiom
Viderе → Recognoscere → Proferre
seeing → recognizing → carrying forward
Mensura. Recognitio. Cura.
Inscription
Liturgia Medica
Officium publicum conservandi ordinem recognitionis,
per quem mensura fit recognitio,
et recognitio fit cura.
the public duty of preserving the order of recognition,
through which measurement becomes recognition,
and recognition becomes care
Brevis Forma
Liturgia Medica
Mensura. Recognitio. Cura.
Measure. Recognition. Care.
Interpretatio
Syndrome – what flows together
Lucerna – where flow is illuminated
Medical – where flow is brought into proportion and recognition
Liturgy – where flow is prevented from dispersing
Clinical epistemic architecture – the systems through which signals of illness are produced, interpreted, transmitted, or fragmented
Circulation – the movement of those signals through that architecture
Recognition – the moment of convergence
Recognition failure – the persistence of signal without convergence
Clavis
Truth may circulate within the system
and yet remain unrecognized.
– C L Gillespie
Mensura. Recognitio. Cura.
What Is Medical Liturgy?
Medical Liturgy is a discipline that studies how truth about illness circulates through clinical epistemic architecture.
Evidence and patient testimony emerge as signals of illness, but these signals must travel through institutional systems before recognition can occur. When circulation succeeds, recognition emerges and care follows. When circulation fractures, recognition collapses even though evidence and testimony remain present. Medical Liturgy therefore examines the structures that allow clinical truth to move, converge, and remain visible long enough for care to occur.
Medical Liturgy expands this premise into a framework for understanding how illness becomes recognizable within healthcare systems. Medicine often assumes that diagnosis follows naturally from evidence, but in practice recognition depends on the alignment of three sources of knowledge: biological evidence, patient testimony, and the institutional structures that process clinical information. These structures — medical records, diagnostic technologies, referral networks, and professional hierarchies — form what Medical Liturgy calls clinical epistemic architecture.
Evidence and testimony must circulate through this architecture before recognition can occur. When that circulation fragments, recognition can fail even when the relevant signals already exist within the system. Medical Liturgy studies these conditions of recognition and the institutional work required to preserve them.
Where Narrative Medicine taught the field how to listen, Medical Liturgy asks how medicine remembers. It begins from a simple but consequential recognition: the modern chart may hear, yet fail to hold continuity long enough for truth to become care. The institution may record, yet still fail to recall. To repair that fracture, medicine requires more than additional protocol. It requires a structure of attention capable of preserving visibility, continuity, and accountability across time.
In that sense, Medical Liturgy is not only analytic but ethical. It concerns the moral and institutional conditions under which evidence remains legible, testimony remains credible, and suffering is not lost in transit. It treats documentation not as clerical residue, but as part of the architecture through which recognition is either preserved or abandoned.
At its most developed, Medical Liturgy becomes a grammar of remembrance within medicine: a way of understanding how witness becomes structure, how continuity becomes responsibility, and how omission becomes a design problem rather than a private tragedy. It understands accuracy as a form of fidelity, continuity of care as covenant, and institutional silence as a rupture that must be named.
Its foundational texts — The Declaration of Patient Fidelity, Testament of the Body, and The Parable of the Forgotten Record — form a triptych of foundation, form, and faithfulness. Together they establish the moral canon of a discipline concerned not only with what medicine knows, but with whether that knowledge can remain intact long enough to matter.
A New Pedagogy of Continuity
If recognition depends on circulation, then continuity must be taught.
Medical Liturgy therefore proposes a pedagogy not of information, but of preservation — training clinicians, scholars, and institutions to maintain the movement of clinical truth across time.
This applied curriculum takes several forms:
• Liturgies of Recall — workshops where clinicians learn to translate documentation into practices of continuity and accountability.
• Ethical Design Labs — collaborations among medicine, law, humanities, and the arts to embed structures of remembrance within systems of care.
• Testament Studios — spaces where patients and scholars reconstruct erased evidence as scholarship, ethics, and policy.
Together, these practices treat continuity not as a byproduct of care, but as its architecture.
The Moral Oath
“I will not allow the record to forget what the body remembers.
I will treat continuity as covenant.
I will design care that endures.”
Purpose & Trajectory
Medical Liturgy does not seek to romanticize suffering.
It seeks to design continuity.
Its purpose is to make remembrance structural — to ensure that evidence, testimony, and recognition remain connected within systems that too easily fragment them.
Through this lens, the patient is not merely a subject of care but a co-architect of evidence.
Testimony becomes infrastructure.
Documentation becomes covenant.
The aim is to replace reactive charting with a pedagogy of fidelity — a living grammar for continuity of care.
Three Pillars of Circulation
The framework advances across three reinforcing domains:
• Legal — accountability through investigation, procedural review, and preservation of record.
• Scholarly — integration into health humanities and ethics as a model for continuity-centered documentation.
• Public — dissemination through essays, visual studies, and discourse that carry testimony beyond institutional boundaries.
Each pillar sustains the others — law granting accountability, scholarship granting continuity, and public discourse granting conscience.
Together they create a field where testimony no longer evaporates when institutions fail to listen.
Toward a Discipline of Witness
As this work circulates within academic, legal, and public domains, it becomes more than a framework.
It becomes a discipline.
Medical Liturgy functions as a living field journal — documenting how individual collapse can become institutional repair.
Within it, the language of faith meets the rigor of evidence, and the act of remembering becomes a structural form of care.
Coordinates of Reinvention
Field Notes from the Edge of Collapse
Coordinates of Reinvention is the living archive of Medical Liturgy — a daily field journal where theory is tested in real time against the moral physics of survival.
Each entry is written from inside the breakdown of a system that forgot how to listen, tracing how a single body’s record becomes a map for institutional repair.
The series began within the Health Humanities Network (HUM) — connecting Columbia, NYU, Harvard, and other programs — as the first applied field journal in the history of the discipline.
In it, lived collapse becomes evidence, and reflection becomes design: a framework where language itself performs the care it describes.
Method
Each reflection follows the same liturgical arc:
• Invocation — attention as devotion.
• Break — the point of erasure or silence.
• Reconstruction — rebuilding language into structure.
• Coda — a single image, phrase, or line that carries forward as a diagnostic of meaning.
These are not essays; they are acts of architecture. They model how a practitioner or patient might translate their own experience into continuity — through form, precision, and compassion.
Light in Vein: Reflections
Reflections from the Practice of Medical Liturgy.
Reflections from the Practice of Medical Liturgy.
A living journal within the field of Medical Liturgy—merging the clarity of a medical archive with the calm of a chapel.
Light in Vein: Reflections gathers writings that trace the moral body of care: moments when observation becomes reverence, and record becomes remembrance.
It invites sustained reading, quiet reflection, and the circulation of care-centered ideas—accessible to clinicians, scholars, and readers alike.
A space where medicine and ethics meet in devotion, restoring attention as the first act of healing.